This page is for my current patients only
此網頁只供我現時病人閱讀

Background 背景
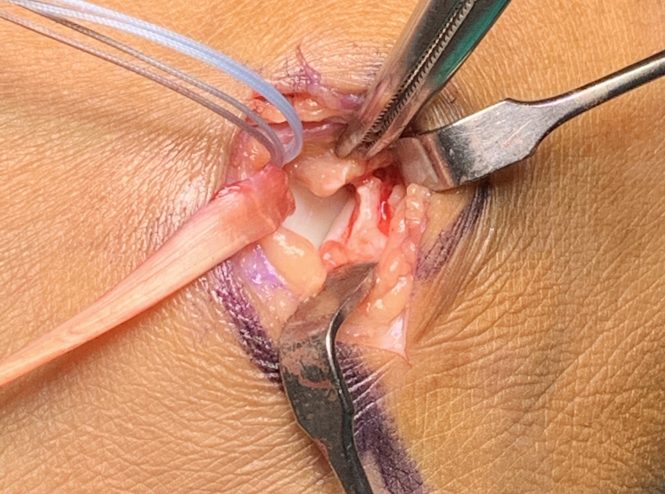
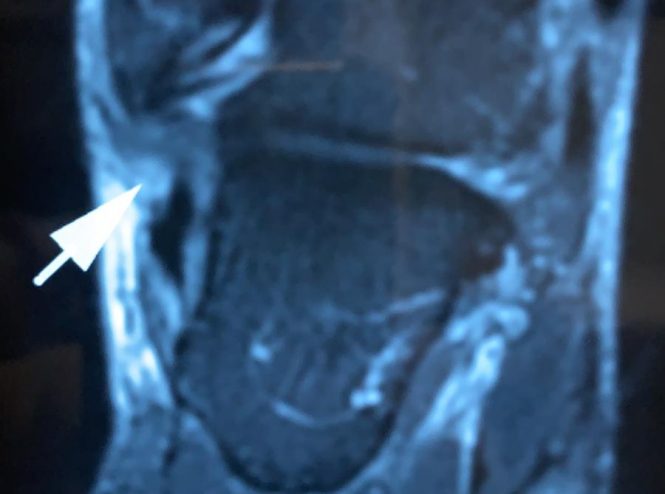
When the Anterior TaloFibular Ligament (ATFL) is torn, an injury commonly happened when one sprains his ankle, the stability of the ankle will be compromised.
While the muscle at the outer side of the calf can partially compensate the loss of the ATFL, in conditions when the calf muscle is in fatigue, or when the strain comes in quick such as stepping into a hole, then the instability will be obvious. It is estimated up to 40% of sprain ankle injury will end up being unstable. Repeated injury can mount to 80% in these cases.
Repeated injury to the ankle not only causes pain and swelling, but also create additional and cumulative injury to the surrounding soft tissue and bone. When the talus is under repeated shearing injury, osteochondral lesion might be resulted, and this lesion is a challenge. Many a time, surgical intervention will be needed, including harvesting one’s own cartilage and transfer to the ankle.
Therefore, when the stability is grossly compromised clinically, Anterior TaloFibular Ligament (ATFL) should be repaired as soon as possible. If left too long, it cannot be repaired, but need reconstruction.
ATFL can be repaired by minimal invasive technique, called full arthroscopic ATFL repair. Open technique however is still commonly practiced because the repair is more secured.
Reconstruction of the Anterior TaloFibular Ligament (ATFL) can be by means of harvesting hamstring and transfer it to the ankle.
After repair or reconstruction, a period of protection is required before the repaired or new ligament regains its strength.
The followings are surgical options, additional procedures, such as Platelet Rich Plasma (PRP), can be incorporated depends on the pathologies facing,
- Arthroscopic ATFL repair
- Open ATFL repair
- ATFL reconstruction
當前距腓韌帶(ATFL)撕裂其實十分常見。當腳踝扭傷(拗柴)時,足踝(腳眼)外側的韌帶必有受傷,問題只是有沒有完成斷掉,如果韌帶斷開,腳踝的穩定性必受影響。
當我們多鍛鍊小腿外側肌肉,或許可補償斷了的前距腓韌帶功能,但當小腿肌肉處於疲勞狀態或如果拉扯發生太迅速,肌肉反應不夠快,例如踏到路上的洞,足踝不穩定性的問題就會變得很明顯。據估計,多達40%的踝關節扭傷最終演變為慢性不穩定 (Chronic instability)。高達80%慢性不穩足踝會重複拉傷。
腳踝反復受傷,不僅會導致疼痛和腫脹,還會令周邊的軟組織和骨骼造成累積性傷害。當距骨反復受到前移拉扯(剪力傷)時,可能會導致骨軟骨病變 (osteochondral lesion),而這種損傷的治療十分困難。很多時候,將需要手術介入,包括抽除自身的軟骨並將其轉移到腳踝,是一個複雜手術。
因此,當臨床彰顯欠缺穩定性時,應盡快修復前距腓韌帶ATFL。如果忽視時間過長,斷開的韌帶將無法修復,需要重建。
我們可以通過稱為全關節鏡前距腓韌帶修復的微創技術修復前距腓韌帶。但是,由於開放性修復更加牢固,因此醫生仍然普遍採用開放技術。
要重建前距腓韌帶,我們需採集膕繩肌的肌腱(大腿後面肌肉,但刀口在膝前方),並將其轉移到腳踝來。
修復或重建後的韌帶強度會逐漸減弱,到4週後最弱,隨後才逐漸恢復強度,所以必須保護6星期。
以下是外科手術的選擇,可根據所面對的病情同時附加其他手術,例如富血小板血漿(PRP),骨固定
- 關節鏡前距腓韌帶修復
- 開啟前距腓韌帶維修
- 前距腓韌帶重建

Indication 適應症
- Anterior TaloFibular Ligament (ATFL) deficient ankle 前距腓韌帶缺失
- Acute traumatic rupture of the Anterior TaloFibular Ligament (ATFL) 急性前距腓韌帶撕裂
- ATFL Tear with fibular avulsion 前距腓韌帶撕裂兼腓遠端骨折
- Anterior TaloFibular Ligament (ATFL) and (CalcaneoFibular Ligament (CFL) tear 前距腓韌帶撕裂兼跟腓韌帶撕裂
- ATFL tear with osteochondral lesion 距腓韌帶撕裂兼距骨軟骨病變
Preparation 預備
- Pre-op workup 手術前身體檢查
- Walking >10000 steps a day 堅持每天1萬步強化背及腿肌
- Do more deep breath 多深呼吸
- Continue usual medication on operative day 手術當天照常食藥
- No food or drink for 6 hours 手術前6小時禁食及禁喝水
- Admit to hospital 3 hours before surgery 手術前3小時到醫院
- Inform your relative despite surgery takes less than 2 hours, you will return no earlier than 3 hours. 通知家人即使手術只需2小時,但回病房可能是3小時後
Risk 風險
While all medical and nursing professionals endeavor to provide best and safest practice, complications still would occur.
General operative risks including heart attack, stroke, wound infection, wound hemorrhage, urinary tract infection, deep vein thrombosis, scar pain, unsightly scar, wound gapping and even failure to heal, etc, is possibly encountered.
Nerve and vascular injury are rarely occurred risk. Risk is higher for older patients. Anatomical variants also carry more risk.
Persistent instability is around 10%. Therefore, early protection and avoid enthusiastic stretching and weight bearing in early stage is important.
儘管醫生和護士都會盡最大努力提供最佳和最安全的治療,但併發症仍會發生。
一般手術可能會遇到的風險,包括心臟病發作,中風,傷口感染,傷口出血,尿道感染,深層靜脈血栓形成,傷口疼痛,外觀不理想甚或傷口不癒等,這手術也不例外。
神經及血管損傷是很少遇上的風險。
老年患者的風險更高。先天結構異常也會有更高的風險。
持續不穩大概為10%。所以早期保護及避免太早活動及受力尤其重要。
Budget Estimation 預算費用
CPT code and RVU is as follows
- 27695 Repair, primary, disrupted ligament, ankle, collateral — is reported for this type of repair when it is associated with an acute injury of the ATFL (anterior talofibular ligament) or CFL (calcaneofibular ligament), RVU 6.7
- 29894 Ankle arthroscopy, RVU 7.32
- 27698 repair, secondary disrupted ligament, ankle,
collateral), RVU 9.61
CPT碼和RVU如下
- 27695,踝關節副韌帶修復—與ATFL(前距腓韌帶)或CFL(跟腓韌帶)的急性損傷相關,RVU 6.7
- 29894 足踝關節鏡, RVU 7.32
- 27698,踝關節副韌帶重建,RVU 9.61
Estimation based on general ward as in Aug-2020,
- Surgeon fee $26,800 (repair), $38,440 (reconstruction)
- Anaesthetist fee $8,933 (repair), $12,813 (reconstruction)
- Ward round $1,200/day
- Hospital charge $60,000
Total $98,133 (repair), $113,653 (reconstruction) around
根據普通房於2020年8月進行的估算,
- 外科醫生費$26,800 (修復), $38,440 (重建)
- 麻醉師費$8,933 (修復), $12,813 (重建)
- 巡房費$1,200
- 醫院費$60,000
- 總計$ 98,133 (修復), $113,653 (重建)
- 左右

Reference figures from private hospitals 醫院提供的參考數據
St Paul’s Hospital 聖保祿醫院
Median Charge 收費中位數
- Doctors’ fee 醫生費 Not provided 未提供
- Hospital charge 醫院收費 Not provided 未提供
- Total 總費 Not provided 未提供
Cannosa Hospital 嘉諾撒醫院
Median Charge 收費中位數
- Doctors’ fee 醫生費 Not provided 未提供
- Hospital charge 醫院收費 Not provided 未提供
- Total 總費 Not provided 未提供
Baptist Hospital 浸會醫院
Median Charge 收費中位數
- Doctors’ fee 醫生費 Not provided 未提供
- Hospital charge 醫院收費 Not provided 未提供
- Total 總費 Not provided 未提供
Adventist Hospital 港安醫院
Median Charge 收費中位數
- Doctors’ fee 醫生費 Not provided 未提供
- Hospital charge 醫院收費 Not provided 未提供
- Total 總費 Not provided 未提供
Post-op care 術後照顧
- Control inflammation with regular usage of anti-inflammatory drug.
- Tighten up your calf muscle inside the cast 10 repetitions every 2 hours when you are awake. After 2 weeks, kneel on the knee of the operated leg on a chair, to allow the thigh to bear weight earlier.
- You are given an cast / cast boot. Please do not remove it as it is intended for holding the optimal position. Therefore you need to wear the cast even when you sleep, sit down or at home. When you go for shower, use a waterproof bag to seal it up.
- Keep your leg up all the time. It should be placed above the chest.
- You should not bear weight on the operated ankle. Use crutches all the time, including at home.
- The wound is covered by a waterproof dressing. After 2 weeks, you can shower after carefully remove the boot temporarily, but do not take bath or rub on it. Keep the dressing intact, there is no need to change it regularly.

- 定時服藥,控制發炎
- 在你清醒時,每2小時在石膏托或固定靴內收緊小腿肌肉10次。你亦應在2星期後開始單膝跪在椅子上,避免大腿長期不承重。
- 你須要保持穿戴提供的石膏托或固定靴。這些固定靴或石膏托,可幫你保持足踝最佳位置。因此,即使在您睡覺,坐下或只在家,也需要佩戴固定靴或石膏托。淋浴時,請使用防水袋將其密封。
- 必須一直保持腿部在胸部上方,以免水腫。
- 剛完成手術的足踝不能受力承重。即使在家也要使用拐杖。
- 傷口已用防水敷料覆蓋。所以2星期後,您可以脫下固定靴淋浴,但不要浸澡或捽這敷料。你只需保持敷料完整,無需定期更換它。
Early Post-op Complication 手術後早期併發症
Notify surgeon in case you have
- Persistent fever of more than 37.5 Celcius
- Chills and rigor
- Wound pain despite rest
- Wound redness and swelling
- Purulent discharge from wound
- Calf pain
- Ankle swelling, progressive
- Sudden onset of shortness of breath
- Chest pain
如發現以下情況,要立即通知醫生
- 持續高燒(口探高於攝氏37.5度)
- 發冷打顫
- 無論運動或休息時,傷口痛楚都持續增加
- 傷口持續發紅腫脹
- 傷口有膿液
- 小腿愈見痛楚
- 小腿、腳踝和腿部腫脹持續增加
- 突發性的氣促
- 胸口突然疼痛


Rehabilitation after Day 14 手術後2週復健
Exercise of calf and thigh muscles:
- Quadriceps contraction:
Sit on chair, with your cast on, straighten the knee, count 15 seconds, and then relax. Rest for 10 seconds and repeat 10 times. - Calf contraction:
Sit on chair, with your cast on, tighten your calf muscle, count 15 seconds, and then relax. Rest for 10 seconds and repeat 10 times.
Load bearing exercise:
- Thigh
With or without the cast boot, kneel with the operated leg on the chair. Shift the body weight to that knee. Stay 10 minutes, . Keep the ankle in air and not moving. - Shin
Sit down, with or without the cast boot, lean forward and press on the knee of your operated leg. Hold 5 minutes, do it 6 times a day, and if no pain, progress to
Put some weight on the knee, such as a young child sitting on the lap, or a slim lady sitting on both laps, 10 minutes, 6 times a day - Whole leg
Stand with the boot on, the other leg on a 2-inch book or brick, to equalise leg length. Then put equal weight on both legs, 10 minutes without moving the ankle. Gradually shift the body weight to the operated side momentarily.
Range of Motion exercise:
- Take off the boot, put the foot on floor, with the forefoot remains on floor. Lift the ankle up, hold 15sec then put heel back on floor. Make sure it is only in planar motion but no varus or valgus motion on ankle.
- From 5th week onward, take off the boot and move ankle up and down but no varus and valgus. To the end range as opposite side.
Further strengthening and return to sports:
- You can sit in the office for a long hours in 4 to 6 weeks after the operation, and go running no earlier than 3 to 4 months.
- Increase the amount of activity gradually and avoid strenuous exercise, especially running, kicking and jumping.
- Sex life can start at 6 weeks after surgery.
- Avoid excessive ankle fatigue within one year.
小腿和大腿肌肉的運動:
- 大腿四頭肌收縮:
坐在椅子上,穿戴着石膏托或固定靴,全神貫注下伸直膝蓋,保持伸直並數15秒,然後放鬆。休息10秒鐘,重複10次。 - 小腿收縮:
坐在椅子上,穿戴着石膏托或固定靴,收緊小腿肌肉,數15秒鐘,然後放鬆。休息10秒鐘,重複10次。
負重練習:
- 大腿
不論是否穿戴石膏托或固定靴,以患肢單膝跪在椅子上。將體重漸轉移到患肢膝蓋上。保持10分鐘。注意腳踝不要移動。 - 小腿
坐下(無論是否穿戴石膏托或固定靴),向前傾用手按患肢膝蓋。保持5分鐘,每天進行6次,如果沒有疼痛,則進展為
每天10次,每天6次,在膝蓋上施加更多重量,例如找個小孩坐在患肢大腿上,或者一位苗條的女士坐在兩邊大腿 - 全腿
穿戴石膏托或固定靴站起來,記得正常腳那邊放一本2英寸的書本或磚頭,以平衡兩條腿的長度。然後在不活動足踝的情況下,把體重平均分到兩條腿,站10分鐘。期間可逐漸將體重短暫轉移到患肢。
- 大腿
運動範圍:
- 脫下石膏托或固定靴,將腳放到地板上,前腳保持在地板上。提起後跟,保持15秒,然後將腳跟放回地板上。注意需確保足踝只作平面運動,而足踝沒有內翻或外翻活動。
- 從第5週開始,脫下石膏托或固定靴,上下移動腳踝,直到活動範圍末端。但不要內翻和外翻足踝。
進一步加強肌力並重返正常運動:
- 您可以在手術後的4到6週返回辦公室坐較長時間。需超過3個月才開始跑步。
- 逐漸增加運動量,避免劇烈運動,尤其是跑步,踢腿和跳躍。
- 性生活可以在手術後6週開始。
- 一年內避免踝關節過度疲勞。
Reference 參考文獻
- Cao Y, Hong Y, Xu Y, Zhu Y, Xu X. Surgical management of chronic lateral ankle instability: a meta-analysis. J Orthop Surg Res. 2018 Jun 25;13(1):159. https://pubmed.ncbi.nlm.nih.gov/29940985/
- Baumbach SF, Braunstein M, Herterich V, Böcker W, Waizy H, Polzer H. Arthroscopic repair of chronic lateral ankle instability. Oper Orthop Traumatol. 2019 Jun;31(3):201-210https://pubmed.ncbi.nlm.nih.gov/30918997/